Tales from the edge of modern fertilities


“Reproduction doesn’t just happen by itself,” says Professor Sarah Franklin, Head of the Sociology Department. “Reproduction is organised, and the way people organise reproduction tells you so much about how they organise everything else.
“Right now, I’d describe fertility as a condensed signifier of precarity. It represents a sense of imperilment. It’s considered ‘something that needs help’, you know?”
Franklin is Principal Investigator of Changing (In)Fertilities, a major interdisciplinary research project funded by the Wellcome Trust ongoing in the Reproductive Sociology Research Group she leads – ReproSoc. The project explores how everything from technology to politics is changing the perceptions and practices of reproduction.
Or, as Franklin puts it, “doing the usual slightly annoying sociological thing of showing people that it’s more complicated than it seems.”
For the past eight years, Franklin has been working with a global network of social scientists looking at a wide range of fertility issues – from western in vitro fertilisation (IVF) clinics to reproductive health in rural Nepal. One key finding is both highly paradoxical and yet somehow intuitive: the more you plan for children, the fewer you have.
"Telling people to go on holiday and make more children for grandma will only get you so far"
Professor Sarah Franklin
“We’re very familiar with the narrative of women having more reproductive options these days,” she says. “But how does that translate into actual experience?
“IVF, for example, is expensive and difficult and nerve-racking. A much-wanted child may result in a desire to provide a sibling, then its back on the IVF track, more time, more money. What’s seen as a solution often creates further problems. We need a better account of the problems the technology is supposed to be solving.”
Franklin uses the example of Cambridge University. “It’s full of talented and powerful women: from undergrads through to postdocs and lecturers, all in the classic position of being prime childbearing age with a demanding work life.”
“What would Cambridge need to do to ameliorate this conflict? More child-friendly spaces, different hours, more attention in the curriculum to childcare realities. Imagine a university designed for a woman in her mid-twenties with two young children – it would be unrecognisable.”
While the 20th century saw fears of overpopulation, birth rates have plummeted in many wealthy nations, and fertility is on government agendas as something under threat, says Franklin. However, the reasons behind these fluctuations are elusive.
The research team is getting under the skin of modern reproduction through what Franklin calls “indicative anecdotes”: case studies that reveal the underlying social drivers behind fertility statistics.
“Resurgent fertility politics needs to be closely watched. It carries ideas about who should have reproduction assisted or curtailed. We want our gallery of situated projects to help show the ways reproduction is deeply implicated in all aspects of life,” she says, “and why the question of causality is so very complex.”
“Policymakers like broad sweeps of applicability, the ‘nudge’, but if there’s going to be meaningful social change, telling people to go on holiday and make more children for grandma will only get you so far.”
Beat the clock
The egg-freezing gold rush


Louise Brown, the world’s first IVF baby, was born in 1978, the culmination of decades of research by Cambridge Nobel scientist Sir Robert Edwards. Since then, an estimated eight million babies have been born globally following IVF and other assisted reproductive technologies (ARTs).
While many different personal journeys have led to these births, there has typically been one unifying rationale: I want a baby, preferably as soon as possible. That’s all changing.
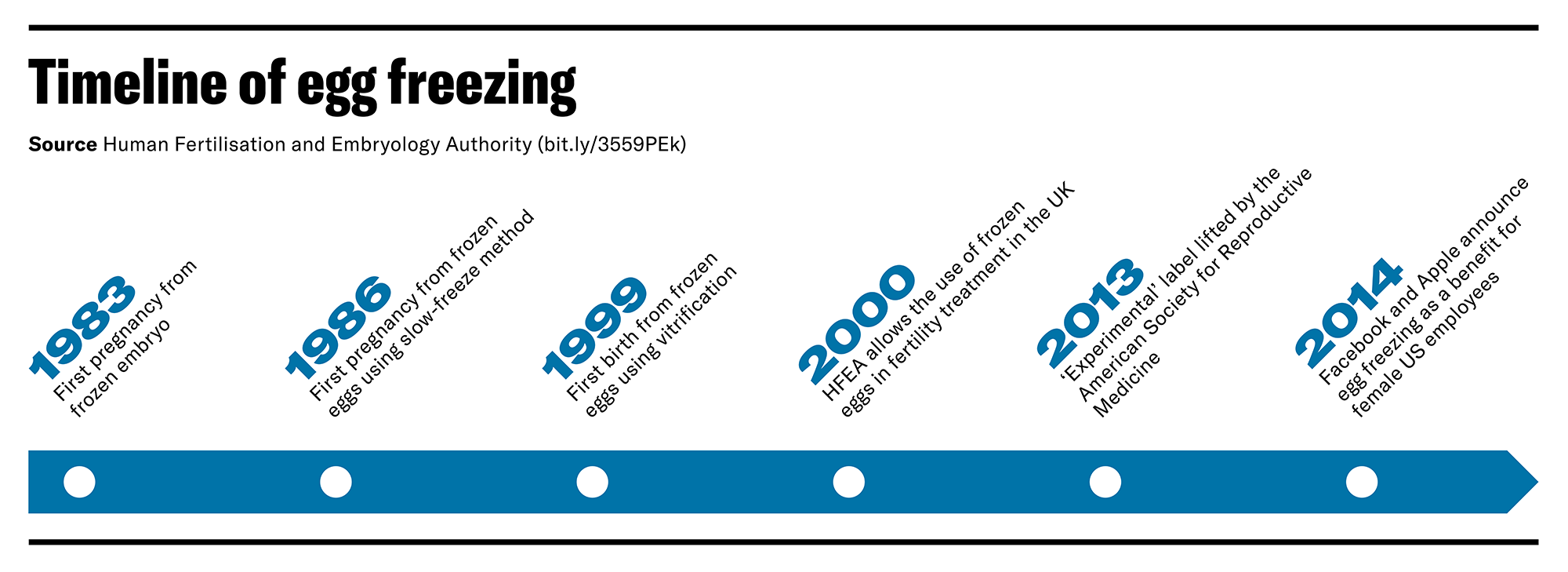
The fastest-growing tech in the reproductive marketplace is ‘oocyte cryopreservation’, or egg freezing. In its early days, it was a resort for women with cancer diagnoses, but very low success rates often led to little more than false promise.
The technology has improved dramatically. An egg is the largest cell in the human body and freezing can cause crystal formation in the cell. Slow-freezing techniques were initially used to circumvent this problem, followed by the more successful flash-freezing ‘vitrification’ that transformed the egg into a glass-like stasis, after which success rates for post-thaw conception jumped.
What became apparent was the potential egg-freezing client base outstripped that of IVF alone, as it included not just women who want a baby, but also all those who might want a baby in the future.
“Egg freezing is both an infertility treatment for the fertile and a fertility treatment for the infertile,” says Franklin’s colleague Dr Lucy van de Wiel, whose research focuses on the explosion in the popularity of this ART. “Increasingly younger women are encouraged to freeze their eggs in preparation for future infertility, and those frozen eggs promise an extension to fertile life.”
By 2013, many of the world’s professional fertility bodies had stopped labelling the treatment as ‘experimental’, triggering a gold rush in egg-freezing investment and marketing. Van de Wiel’s book Freezing Fertility, published by New York University Press, tracks this rapidly expanding offshoot of the fertility industry, and the people it aims to attract.
“We’ve always had commercialisation of IVF, but there’s a large amount of private equity and venture capital investment pouring into egg freezing – often coming from places with no links to the fertility industry,” says Van de Wiel.

Start-ups focusing on clinical freezing services are seeing such an influx of capital that they are acquiring many established independent IVF clinics, creating corporate fertility franchises unlike anything previously seen.
The target customers for these new conglomerates are not just women in their mid-thirties but those a decade younger. And the marketing pitch isn’t a newborn babe, but rather freedom and reproductive control.
“Look at Prelude, founded by an IT entrepreneur,” says Van de Wiel. “Within two years they had bought dozens of clinics across the USA, and now claim to be the country’s largest fertility company. Much of their marketing depicts single young women, not families with babies.
“Their pitch to women is: freeze your young eggs, use our extra testing, so you have the best genetic material for making a baby when the time is right for you. Feel reassured that you can live free from your body clock, because meeting the right partner at the right age and conceiving through sex is too unpredictable.
“Their pitch to investors is: with our treatments, people can have children when they are ready, even if that is at a time when they are no longer fertile. Combined with fertility demands for same-sex couples, it’s a market set to increase – and one likely to stay strong in economic downturns. Children are priceless; people are willing to spend a lot to have them.”

A section of the Prelude homepage.
A section of the Prelude homepage.
She adds: “While the average age of a woman freezing eggs in the UK is still 37, there is an idea increasingly sold that the younger you do it the better. I’ve heard about fertility preservation stalls at graduate fairs.”
Freezing can lock women into a financial cycle. Eggs need to be stored, which means regular payment, ranging from upwards of £200 annually in the UK to over $1,000 in the USA. The more eggs, and the more cycles, the higher the chances of conception down the line. Some countries impose a shelf life – eggs are destroyed after 10 years in the UK.
The new industry has got this covered. Some start-ups specialise in fertility loans or subscription plans. In the USA, fertility insurance packages that include egg freezing are used by employers to attract the best female graduates or executives.
The expansion of ARTs can create “new forms of dependency,” says Van de Wiel, as well as reproductive anxieties in women from younger ages. “Certain demanding careers may come to be seen as contingent on ARTs such as egg freezing if women entering them want the option of children. To have a healthy child at the best time, women can become reliant on companies to test their fertility, or preserve and store their eggs, or implant a healthy, tested embryo.”
Van de Wiel says she’s all for technologies such as egg freezing, “but it’s important to stay well informed, and not just about the biological facts, but also the business structures you’re participating in.”
Birth Debt
The UK's underground maternity economies
Access to ARTs relies on access to capital: money makes many babies in the 21st century. But poor women in rich nations still want children, still get pregnant, and still need maternal care. In the UK, we might like to think this is a basic right afforded to all women regardless of status or bank account. We’d be wrong.
Dr Kathryn Medien is investigating what happens when aspects of the UK’s border policy, what some call the “hostile environment”, are inserted into maternity care. In 2017, the introduction of healthcare charges for migrants in Britain means that if it isn’t GP or A&E, it costs, and that includes having a baby.
Medien has been unpicking some of the mechanisms behind these charging systems, from data sharing between the NHS and Home Office to digital footprint checks. She argues that it marks a financial transition in British healthcare, a “privatisation of the underclass”, and one that could be extended post-Brexit.
“It’s easy to become a visa overstayer,” says Reprosoc researcher Medien. “Visas cost thousands of pounds, and few people have that. Certainly not woman who arrive to marry a man who becomes abusive, or abandons them, when pregnant. Or soon-to-be-mothers with failed asylum claims, or yet to be processed claims.”
“All the preliminarily studies on healthcare charging on the UK suggest that it disproportionately affects women due to give birth. It’s not an ailment you can choose to ignore – that baby’s coming out of you, and you need medical help.”
Charging those deemed to be “not ordinary residents” for secondary care – including maternity – is “profit-making” says Medien, as it comes in at 150% the cost of care. If the debt is over £500 and outstanding for two months, details pass to the Home Office, and any hope to remain in the UK can be lost as a result.
"There is a closing down of reproduction opportunities for poorer migrant populations"
Dr Kathryn Medien
Consequently, many women fear hospital visits when pregnant. Hospitals now have an obligation to question those they suspect of residing in the UK “illegally”, so women that do initially seek maternity care are often scared to return.
This has led to an increase in informal networks within migrant communities – Medien talks of “underground economies of birthing” – that provide women with maternal care, often in a more holistic way than the NHS is able to provide.
Medien has been conducting interviews with doulas, or birthing companions, who work either pro bono or through small charities in North London and Birmingham. “There’s a long tradition of doulas in Britain, often considered something for the middle-classes, but many work to help migrant or incarcerated women.”
Doula is the latest word to describe the ancient tradition of a birth companion who provides a mother-to-be continuity of support throughout the process. “Some doulas talked about training to be midwives, but being put off by the pressures within the NHS, which they felt didn’t allow them to provide the right level of care,” says Medien.
The doulas recounted seeing more and more women arriving extremely late to community centres to access help, so not receiving support during pregnancy. “One the first questions a doula is often asked is ‘can you help me with a hospital payment plan?’ such is the fear of debt collectors or deportation.”
Medien is building a dataset of charging for maternity care across the NHS using Freedom of Information requests, starting in London. Early findings show that while the King's College Hospital NHS Foundation Trust raised 267 maternity invoices in between April 2018 and March 2019, the Whittington Health Trust raised fewer than five.
The culture within each hospital often dictates who gets charged and how, says Medien. Trusts have overseas officers expected to question patient immigration status, and some are more eager than others. Many doctors and midwives refuse to comply with passport-checking directives, supported by collectives such as Docs Not Cops.

A poster from a campaign by Docs Not Cops.
A poster from a campaign by Docs Not Cops.
Last year, controversially, Greenwich and Lewisham NHS Trust was found to be using credit check company Experian to comb through digital records and uncover suspected migrants receiving care. This has since stopped and an inquiry launched.
After two months without a payment plan, details are passed not just to the Home Office but debt collection agencies. Medien found the most common agency used is CCI Credit Management, who boast offices in over 90 countries where they can chase NHS debt.
“A lot of practitioners are very concerned that this is eroding principles of universal healthcare in Britain,” says Medien. “Vulnerable women with newborns, who are living in hostels or sofa-surfing, are being chased for maternity payment running to thousands. Bailiffs appearing on doorsteps.”
She argues that, while this case study is UK-based, it’s part of a global trend. “The proliferation of ARTs means an increased ability to reproduce for populations who couldn’t before – whether that’s LGBTQ people, or single or older women – so long as they are wealthy enough.”
“At the same time, there is a closing down of reproduction opportunities for poorer migrant populations, those fleeing war or economic hardship.” For many women, reproducing means incurring debt, whether to extend fertility or get maternity care. “It raises the question of just who gets to access reproduction?” says Medien.
Read more about our research into all aspects of reproduction in Horizons (PDF), the University of Cambridge's research magazine, and find related articles online.
Cambridge Reproduction Strategic Research Initiative
From understanding ancient ideas of generation to exploring new frontiers in fertility, Cambridge researchers are working across disciplines to study reproduction from multiple perspectives. For more information, visit the Cambridge Reproduction Strategic Research Initiative website.
Image credits:
Top image: Cryocanes, used to store frozen human reproductive cells, credit: Gina Glover
Beat the clock image: A human oocyte, credit: ZEISS Microscopy
Birth debt image: ultrasound of a human foetus, credit: Nevin Dilmen

{kind=link}