Predicting better
How two websites are transforming outcomes for breast and prostate cancer patients


Impact at a glance
- Cambridge cancer specialists developed PREDICT Breast and Prostate, the leading online risk communication tools for these diseases.
- Built with the University’s Winton Centre for Risk & Evidence Communication, the two websites have helped thousands of patients across the world reach better clinical outcomes, avoid unnecessary treatments and experience less distress.
- PREDICT is used in more than 200 countries and has had over two million visits.
- In the UK alone, PREDICT has helped the NHS save millions of pounds.

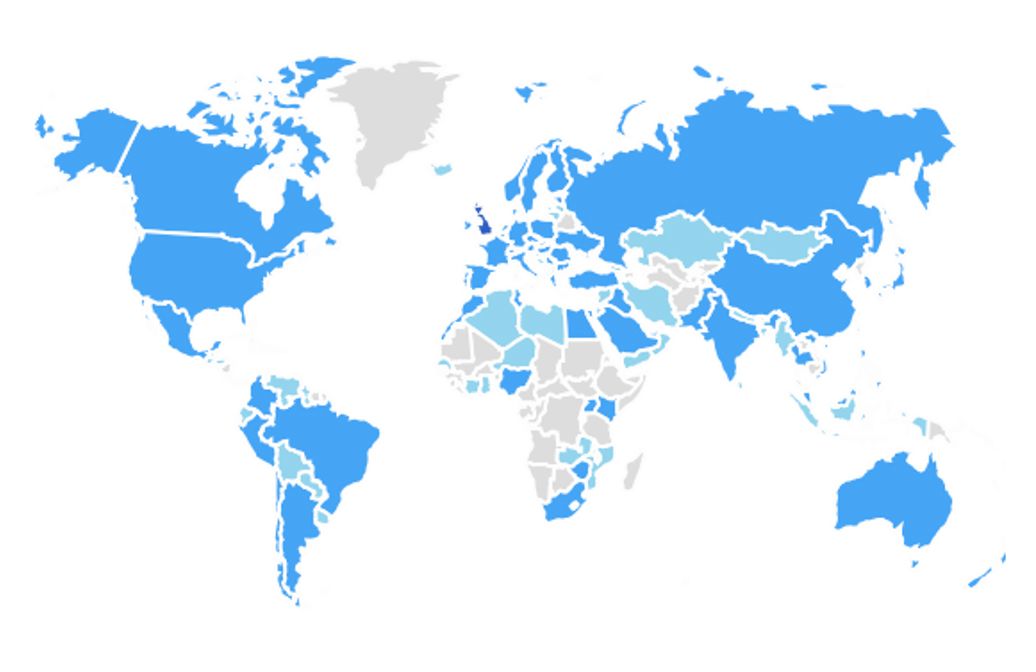
PREDICT's use across the world as of April 2021. Darker blue indicates higher usage.
PREDICT's use across the world as of April 2021. Darker blue indicates higher usage.
“A prediction model is only useful to clinicians if it actually helps them make a decision.”
The problem
After a cancer diagnosis, patients and doctors try to reach an informed decision about which treatment options will provide the greatest chance of extending or increasing quality of life. This conversation ought to consider both the benefits and harm which treatment could bring about. Until recently, very few tools have been available to support this critical process.
Breast cancer is the most frequent cancer among women, affecting over two million each year. Women with early breast cancer often face an agonising decision of whether to have supplementary (“adjuvant”) chemotherapy, treatment given in addition to surgery, with the aim of stopping the cancer returning.
Some women go on to suffer over-treatment by undergoing invasive and unpleasant therapy that will not increase their survival chances. Others become victims of under-treatment, going without therapies that might have improved their outcome.
Prostate cancer is the second most common cancer in men, with around 1.3 million global cases each year. Immediate radical therapy for many of these patients carries a high risk of severe adverse effects, including incontinence, impotence and bowel dysfunction, while providing little therapeutic benefit.
Determined to improve outcomes for these men and women, Cambridge researchers developed PREDICT, a pair of powerful online ‘risk communication’ tools which facilitate informed treatment decision making.
Hosted by Public Health England at breast.predict.nhs.uk and prostate.predict.nhs.uk, the value of these free-of-charge tools has been recognised by clinicians, patients, policy-makers and professional organisations worldwide. By improving the targeting of treatment, PREDICT has contributed towards better clinical outcomes in many parts of the world, as well as reducing patient distress and reducing unnecessary healthcare procedures.
PREDICT Breast
In 2010, Paul Pharoah, Professor of Cancer Epidemiology at Cambridge, developed the first version of an online tool to help healthcare professionals and their patients understand how different treatments for early invasive breast cancer might improve survival rates after surgery.
“In 2007, we were talking in the Cambridge Breast Unit about how they made chemotherapy decisions,” Pharoah recalls. “They used a tool which they didn’t like much because it was based on US data. I suggested that we could do something similar with UK data. They were a bit surprised I was prepared to give it a go but that’s how it started.”


Professor Paul Pharoah
Professor Paul Pharoah
Working with a PhD student, Pharoah began by analysing survival data for 5,700 women with early breast cancer treated between 1999 and 2003. This research made it possible to identify key predictors of survival and the production of a prognostic model which went on to be validated with independent datasets from England and Canada.
Pharoah says: “The project wasn’t properly funded. My PhD student and I worked on it at weekends, and the first version of the webpage was built by a biometrician in my group, again in his spare time. It was ‘wing and a prayer’ stuff.”
“There are a lot of prediction models out there, many of which never get used. We’ve probably had some luck but I also have an unusual set of skills. I was a clinician before training in public health, and then in epidemiology so I understood that a prediction model is only useful to clinicians if it actually helps them make a decision.”
Initially, the Cambridge Breast Unit used PREDICT Breast in parallel with their previous tool but after a year they dropped that. Other breast units heard about PREDICT and the project expanded organically from there.
An evaluation of PREDICT Breast 1.0 in a cohort of women aged 40 years at time of diagnosis revealed that it offered accurate long-term prediction of outcomes for younger women but gave less accurate short-term predictions. In particular, the model was inclined to underestimate short-term (five-year) survival for younger women. Among older patients, it accurately predicted five-year overall survival, but slightly overestimated ten-year overall survival.
Determined to improve the model and website, Pharoah submitted a funding application but was turned down. “The committee didn’t think it was going anywhere. I would love to get them around the table now and point out that PREDICT has had over two million users.”
Continuing to work on the project, Pharoah was contacted by a Brazilian clinician, Francisco Candido dos Reis, who said he had been using PREDICT in Sao Paulo Province and wanted to come and work with him for couple of years.
Candido dos Reis helped to develop an improved model which, among other additional factors, took into account age at diagnosis. PREDICT 2.0, completed in 2017, now reliably characterises relationships between survival and initial tumour size, and whether the cancer has already spread to lymph nodes in the armpit. It is, multiple independent data sets have confirmed, significantly more accurate in estimating the number of breast cancer deaths and cancer-specific mortality in younger women.
Around the same time, Pharoah was approached by Professor Sir David Spiegelhalter, who was then establishing the Winton Centre for Risk & Evidence Communication. Spiegelhalter admired PREDICT’s statistical model and asked if his team could help develop the website.
Pharoah says: “Our original tool was very easy to use but as we added things to the model, it would have become less so. The Winton Centre helped us to overcome that challenge but they also showed us how people like to be presented results in different ways so instead of just giving one kind of graph, we started offering more options.”
The first page of the PREDICT Breast tool
Example chart generated by the PREDICT Breast tool showing a 93% survival rate at 10 years after surgery only.
Example curve generated by the PREDICT Breast tool showing a 93% survival rate at 10 years after surgery only.
Example icons generated by the PREDICT Breast tool showing a 93% survival rate at 10 years after surgery only.
PREDICT Breast is now used in more than 200 countries and has had over 1.25 million visits since 2014. In 2018, PREDICT Breast became the only tool recommended by UK National Institute for Health and Clinical Excellence (NICE) for planning the use of adjuvant therapy for breast cancer and the management of early and locally advanced disease. NICE recommend the use of PREDICT Breast for all patients with early breast cancer prior to other advanced molecular profiling.

In the breast units of most UK hospitals, PREDICT Breast has been adopted as the clinical management decision tool of choice. It has already been used with well over 100,000 women in the UK, of whom at least 18,500 have been able to make better decisions about whether or not adjuvant chemotherapy is right for them.
A clinical review of 200 patients managed by the Cambridge Breast Unit found that 7.5% of patients who would have been classified as low risk and not offered chemotherapy, were classified as high risk by PREDICT Breast and offered chemotherapy. Conversely, 11% of patients who would have been classified as high risk and offered chemotherapy, were reclassified as low risk and spared chemotherapy.
A conservative estimate suggests that since 2013 in the UK, PREDICT Breast has resulted in around 7,500 women being offered chemotherapy who would otherwise not have been, and around 11,000 women being spared unnecessary chemotherapy.


Across the world, PREDICT Breast is helping thousands of women reach better decisions about their treatment after surgery. Image: FatCamera
Across the world, PREDICT Breast is helping thousands of women reach better decisions about their treatment after surgery. Image: FatCamera
Pharoah says: “Clinicians tend to overestimate risk, they’re more likely to prescribe chemotherapy if they don’t have a tool to estimate. There are good reasons for that – if you have 100 patients and for the sake of argument 80 of them are cured, and 20 come back with recurrence, you’re going to remember those 20 and forget the 80 that don’t come back. So your perception of risk is much higher than it actually is.”
According to NICE, adjuvant chemotherapy costs tens of thousands of pounds per woman treated so by sparing thousands of women unnecessary chemotherapy, PREDICT has already helped the NHS save many millions of pounds.

Many women with breast cancer use the tool themselves to better understand their own risk, enabling them to be more informed in their discussions with oncologists about treatment options. Patients regularly discuss the PREDICT tool and share personal experiences on the Breast Cancer Now patient forum and an online survey conducted by the Winton Centre found that women generally favoured taking part in the decision-making process and understanding the risks involved.
Pharoah says: “Joint decision-making is better than it was 20 years ago but this varies enormously around the UK and around world. In many places, doctors still tell patients that they are prescribing chemotherapy. We don’t prescribe chemotherapy, patients choose whether or not to have it. Once the rationale for a decision is made more explicit because it’s based on a number, clinicians are more likely to have a proper discussion with their patient.”
Thanks to its open access model, PREDICT’s extraordinary impact has gone far beyond high-income countries. A 2019 survey of 100 breast cancer oncologists in India found that 58% reported using PREDICT for adjuvant decision making, and 94% felt that it could be used as an alternative to genomic tools in resource-constrained settings. Versions of PREDICT have now been released in French, Spanish, Dutch, Portuguese and in September 2021, both traditional and simplified Chinese.
PREDICT Prostate
Building on the success of PREDICT Breast, between 2016 and 2019 Cambridge researchers developed PREDICT Prostate, the first online resource for individualised treatment decision making in the management of non-metastatic prostate cancer.
While PREDICT Breast examines the value of adding chemotherapy or additional hormonal therapy after surgery, PREDICT Prostate asks a more basic question: should we treat at all or just monitor?”
More specifically, the tool provides patients with estimated survival rates after treatment in the context of absolute mortality rate, which allows patients to make an informed decision as to the value of treatment and its potential side effects.

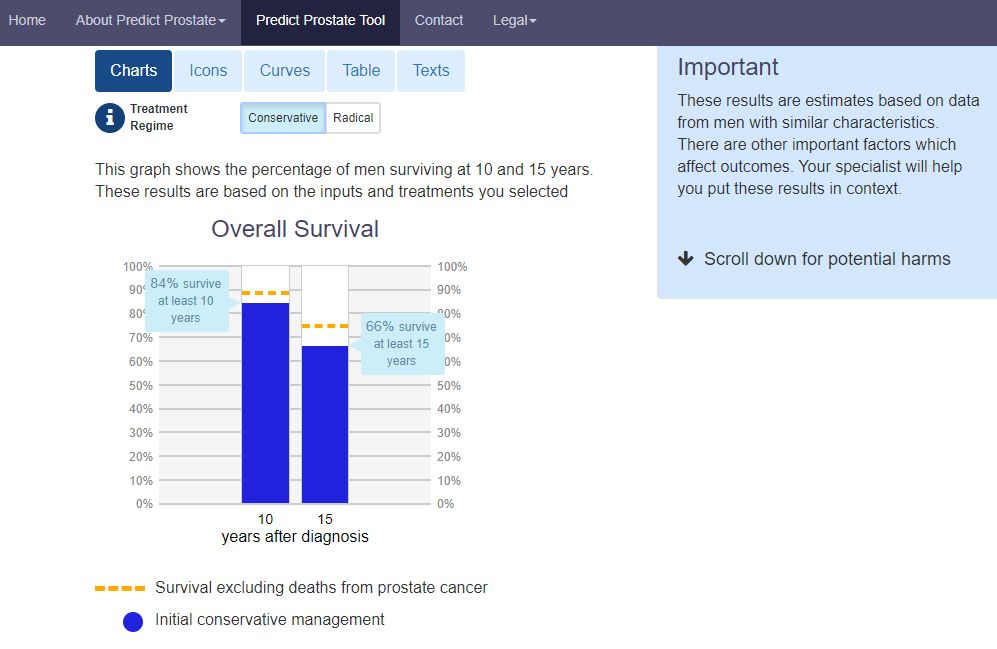
Example chart generated by the PREDICT Prostate tool showing 84% survival rate at 10 years and 66% at 15 years with a conservative treatment regime.
Example chart generated by the PREDICT Prostate tool showing 84% survival rate at 10 years and 66% at 15 years with a conservative treatment regime.
Vincent Gnanapragasam, Professor of Urology at Cambridge and Honorary Consultant Urologist at Addenbrooke’s Hospital said: “When I started out over a decade ago, the mantra was that prostate cancer needs to be treated. The tools which we were using, which are still in use, are pretty crude so many men categorised as low and intermediate risk were receiving treatment which wasn’t beneficial.”


Vincent Gnanapragasam
Vincent Gnanapragasam
Gnanapragasam started working with the then East of England Cancer Registry to better understand treatment trends and co-developed ‘the Cambridge Prognostic Groups’, a five-tiered prognostic classification system to better discriminate cancer-specific mortality in men diagnosed with primary non-metastatic prostate cancer.
The system proved a powerful tool but it still wasn’t possible to give individual predictions. Gnanapragasam was trying to work out how to achieve this when, in 2017, he met Paul Pharoah at a conference and heard about the work he was doing on PREDICT Breast. After that discussion, they started working together.
Using data from over 12,000 prostate cancer patients in two international cohorts, the team – including Gnanapragasam’s “exceptional” PhD student, David Thurtle – developed a model which estimated 10- and 15-year survival outcomes for men with newly diagnosed prostate cancer.
A validation study involving more than 69,000 men showed that PREDICT Prostate was more effective at predicting outcome and the need for treatment than any other models.

In a randomised trial performed between 2018-20 with 145 newly diagnosed men in the UK, 57% reported that the PREDICT Prostate estimates for prostate cancer–specific mortality (PCSM) were lower than expected, and 36% reported being less likely to select radical treatment. The study, recently published in the journal European Urology, found that PREDICT Prostate reduces decisional conflict and uncertainty, and shifts patient perception around prognosis to be more realistic.


A study conducted amongst clinicians showed that PREDICT Prostate reduced the likelihood of recommending radical treatment to patients by around 60%. The complete removal (prostatectomy) or radiotherapy of the prostate currently costs around £7,000 in the UK even before the management of subsequent common side effects such as incontinence, erectile failure and bowel dysfunction. Based on these estimates, the use of the PREDICT Prostate tool in routine practice could potentially save the NHS over £40 million per year in unnecessary radical treatment costs.


PREDICT Prostate significantly reduces the likelihood of patients being recommended surgery. Image: Ahmad Ardity from Pixabay
PREDICT Prostate significantly reduces the likelihood of patients being recommended surgery. Image: Ahmad Ardity from Pixabay
Gnanapragasam says: “I used to do prostate removal surgery but became less convinced that we were doing much good for a lot of patients. That isn’t to say that surgery is not beneficial but in the early days, we were operating on an array of cases in which the cancer was never going to become problematic but we did not have reliable ways to say who would and would not.”
“If somebody makes a decision to have surgery or radiotherapy, and they experience these side effects fully informed up-front and they have realistic expectations, then these things are more acceptable. But if you have something done that probably didn't need doing, that is very hard to cope with.”

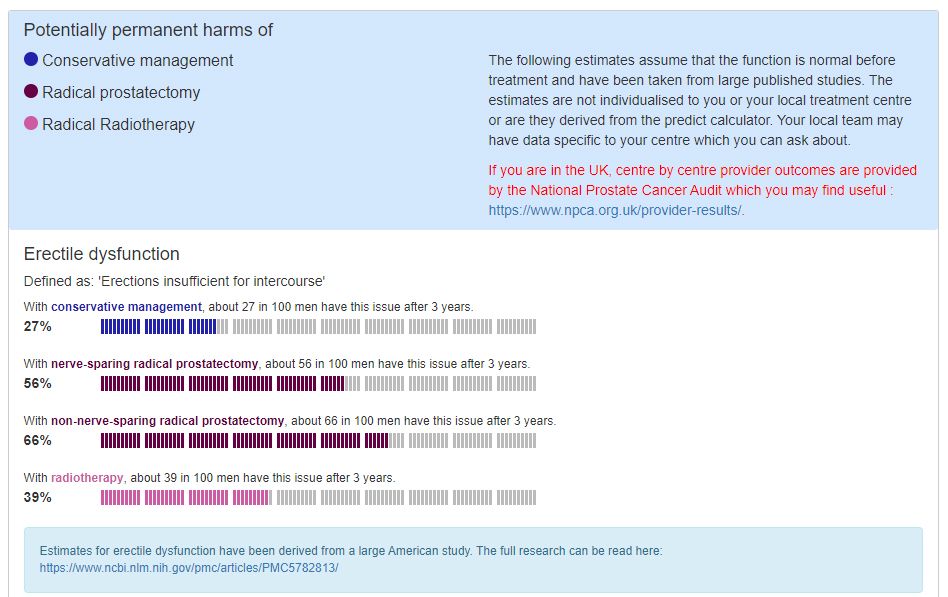
Part of a chart generated by PREDICT Prostate showing estimated potentially permanent harms of conservative management, radical prostatectomy and radical radiotherapy.
Part of a chart generated by PREDICT Prostate showing estimated potentially permanent harms of conservative management, radical prostatectomy and radical radiotherapy.
Gnanapragasam says: “In the past, if a patient saw a urologist who did prostate removals then they were more likely to get their prostate removed. If they saw an oncologist who did radiotherapy to the prostate, they were more likely to get radiotherapy. If they saw somebody who likes to monitor, then they were more likely to get monitoring. That’s an unacceptable variance which shouldn't exist.
“When we use PREDICT, when we show patients the numbers and the figures, that puts a firm boundary around the benefits of treatment. For the patient, knowing exactly what we are talking about and having that consistency, provides a lot of reassurance.”

PREDICT Prostate reduces decisional conflict and uncertainty. Image: undefined undefined
PREDICT Prostate reduces decisional conflict and uncertainty. Image: undefined undefined
PREDICT: The Future
Gnanapragasam expects PREDICT to evolve by harnessing advances in AI so that the predictive tools can adapt to an individual patient’s condition as it develops. There may also be scope to help with other cancers. Just as PREDICT is applied differently for breast and prostate cancer, any new tools would need to respond to specific questions posed by the disease.
Pharoah says: “These tools only get used if they are designed to address a specific clinical decision that’s problematic. A PREDICT tool can’t help make decisions for ovarian cancer because everyone gets chemotherapy unless they're too sick to tolerate it. But it might prove useful with melanoma and colorectal cancer, for instance, where there are difficult chemotherapy decisions to be made.”
The development of such tools would not require huge sums of money but the project remains in need of secure long-term funding. “Given how widely PREDICT is used and the extraordinary impact it’s had and continues to have, that’s astonishing,” says Pharoah, steadfast as ever.


Published 21st October 2021
Infographics by Alison Fair. Laptop images by Tom Almeroth-Williams

... visit our interactive map to find out how.
