COVID-19
The long view
History suggests that this pandemic will be a short-term interruption to long-run improvements in life expectancy, which should resume within a few years.


This is an abridged and simplified version of Leigh Shaw-Taylor’s Introduction to the Economic History Review’s selection of articles on the history of disease, epidemics and improvements in life expectancy, which is currently open access here.


With several billion people currently in lockdown the history of infectious diseases has a new relevance. The topic may seem morbid, but is a fundamentally optimistic one.
In 2019 global life expectancy was approaching 73 years. In 1800 it was probably about 30. This is arguably the most important single historical change of the last 200 years. In 1800 no country in the world had a life expectancy much above about 40.


Today most people in rich countries die of degenerative diseases or complications arising from them, such as cancer, heart disease, diabetes and dementia. In the past the majority of people everywhere died from infectious diseases and only a minority lived long-enough to succumb to degenerative diseases.
Even in major famines, before the twentieth century, most deaths were from infectious diseases, triggered by the changes in behaviour induced by famine conditions.
Today in rich and middle income countries most deaths occur amongst the elderly, while deaths in infancy and childhood are increasingly rare. COVID-19, with the possibility of sudden infection leading to serious illness and even death (in a small percentage of cases) for adults who are neither elderly nor frail sounds a faint echo of an earlier world, in which death from infectious disease, at any age, was an ever-present risk.
Whilst life expectancy and infant mortality rates vary considerably around the world today, nowhere has a life expectancy as low as, or an infant mortality rate as high, as late Victorian Britain, which then had one of the world’s highest life expectancies.
In 2018 the infant mortality rate ranged from as low as one per thousand in Finland to as high as 85 in the Central African Republic. In England and Wales between 1876 and 1900, then one of the most affluent nations on earth, 149 infants out of every thousand born, died in the first year of life.
With an estimated life expectancy of 52.8, the Central African Republic may have come last in global rankings in 2018, but this still looks better than the UK in 1900 with a life expectancy of 46, and far better than England in the early eighteenth century with one in the mid-thirties.
The fundamental nature of this change is clear if we look at mortality before 1900. Thanks to work over several decades at the Cambridge Group for the History of Population and Social Structure, we understand the long run trends in mortality and life expectancy in England over nearly five centuries – far longer than for any other country on the planet.

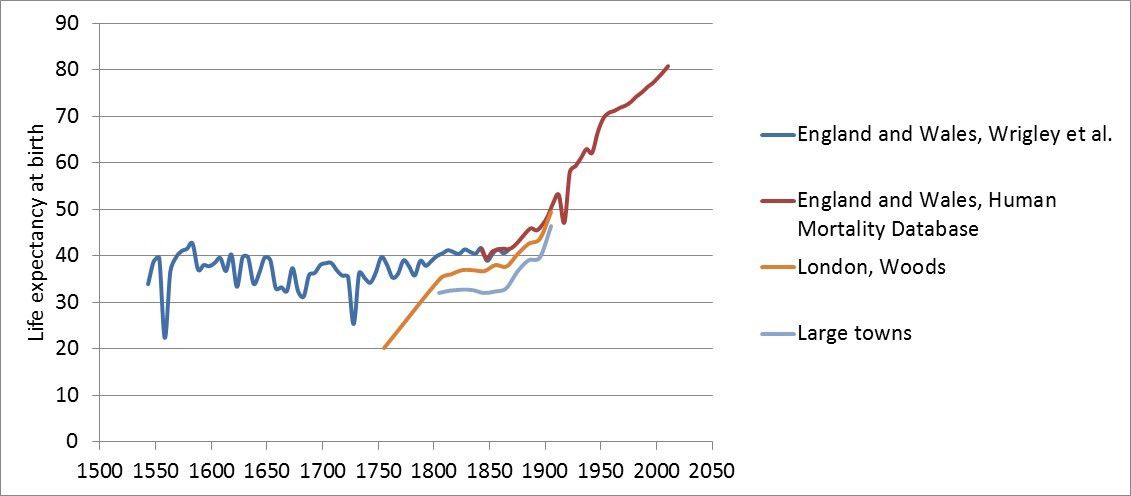
Figure 1: Estimates of long-run life expectancy at birth in England 1543–2011 . Data for England & Wales 1543–1868 from E.A. Wrigley & R.S. Schofield, The population history of England 1541–1871: a reconstruction (Cambridge, 1989). The later nationwide series is from the Human mortality database. The urban and London series are from R. Woods, Demography of Victorian England and Wales (Cambridge, 2000).
Figure 1: Estimates of long-run life expectancy at birth in England 1543–2011 . Data for England & Wales 1543–1868 from E.A. Wrigley & R.S. Schofield, The population history of England 1541–1871: a reconstruction (Cambridge, 1989). The later nationwide series is from the Human mortality database. The urban and London series are from R. Woods, Demography of Victorian England and Wales (Cambridge, 2000).
The spectacular long-run increase in life expectancy visible in figure 1, which Richard Easterlin termed the mortality revolution, has been brought about by fundamental shifts in the causes of death. To understand the origins of this transition in England, we have to look at the historical sequence by which so many causes of premature death have been vanquished over time. That story began around 1600.
Patterns of death we have escaped
In the nineteenth century, around half of all deaths were from infectious disease and non-communicable conditions were far less important than in rich countries today.
Between 1848 and 1872 tuberculosis was the leading cause of death in Britain, accounting for 15% of all deaths. By contrast heart disease, strokes etc., accounted for only 5.8% of reported deaths and cancer for a mere 1.7%. Because so many people died at relatively young ages relatively few lived long enough to develop life-threatening heart disease or cancer.
In England in 2016, only 3% of people died before the age of 50 and more than half lived to 80 or more. By contrast, in a sample of English villages and small market towns in the 1640s, 30% of all children born died before their tenth birthday. Mortality in the first year of life was especially severe – less than half of those born made it to their 45th birthday.
The differences between the two curves in figure 2 are largely explained by rising living standards, public health measures and medicine, which amongst other things, reduced the direct and indirect effects of infectious diseases.

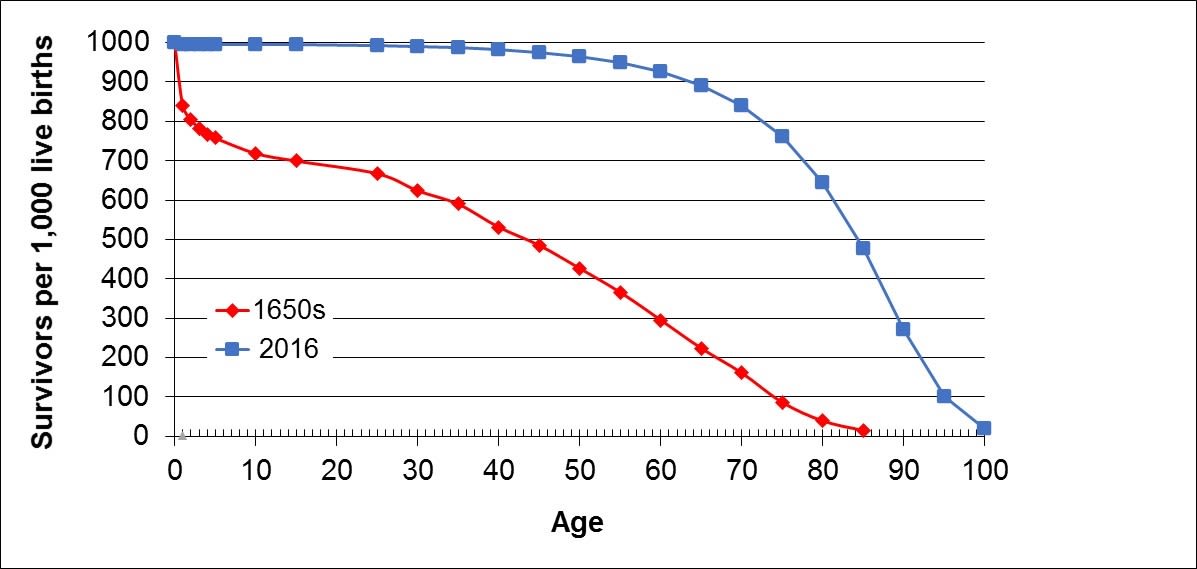
Figure 2: Cohort survival curves for England 1650 and 2016. The data for 1650 are based on a sample of reconstituted parish populations in 1650–9: Wrigley et al, English population history from family reconstitution 1580–1837 (Cambridge, 1997). The 2016 data is from the Human mortality database.
Figure 2: Cohort survival curves for England 1650 and 2016. The data for 1650 are based on a sample of reconstituted parish populations in 1650–9: Wrigley et al, English population history from family reconstitution 1580–1837 (Cambridge, 1997). The 2016 data is from the Human mortality database.
Everywhere in the world, until the late nineteenth century, urban mortality was higher than rural mortality. In Europe and North America in the eighteenth century, an excess of deaths over births in urban areas was the norm. Yet by 1800, as figure 3 shows, London – on the way to becoming the largest city the world had ever seen – achieved a balance between births and deaths, and in the early nineteenth century births came to exceed deaths.
The trend towards an excess of births over deaths appears to have been a general feature of urban centres in England and at least some cities elsewhere in the late eighteenth and early nineteenth centuries.
By 1800 the beginning of the mortality revolution was underway.
Without this epidemiological transition, modern economic growth and the massive urbanisation that took place first in nineteenth-century Britain, before spreading across Europe, North America and Japan, and in more recent times to all inhabited continents, would not have been possible.

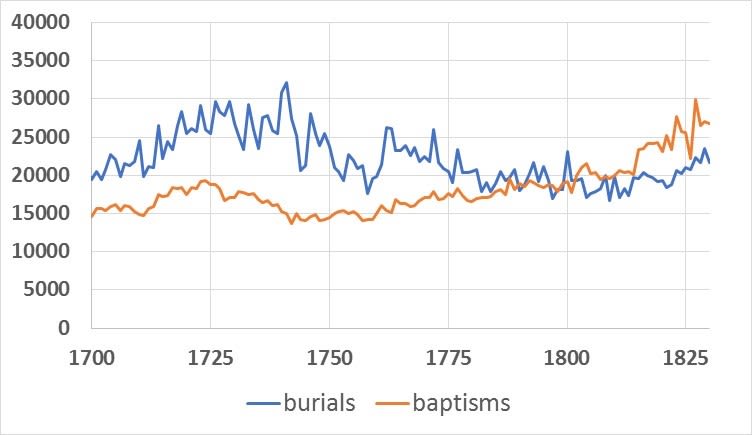
Figure 3: Recorded burials and baptisms in the London Bills of Mortality 1675–1830. Data from J. Marshall, Mortality of the metropolis (1832), pp. 67, 70–1.
Figure 3: Recorded burials and baptisms in the London Bills of Mortality 1675–1830. Data from J. Marshall, Mortality of the metropolis (1832), pp. 67, 70–1.
Escape from famine and plague
In England, the earliest success in the escape from premature death was the escape from ‘the spectre of famine’, which occurred a century earlier than in most of Western Europe and a quarter of a millennium before Ireland.
1623–4 appears to have seen the last geographically extensive famine in England. But it is very unlikely that in this or previous famines large numbers of people starved to death. Responses to harvest failure triggered epidemics and most excess mortality was from infectious diseases.
The first pathogen successfully defeated by human action in Europe was plague (Yersinia pestis, a bacterial infection), which is believed to have killed between one and two thirds of its population between 1347 and 1352.
Plague, a vastly more lethal pathogen than COVID-19 with case fatality rates which may have been 60–90%, was probably defeated by the development of relatively simple but stringent surveillance and quarantine measures.
In Europe, systematic quarantine, cordons sanitaire and public health measures, including contact tracing, were first developed in the Renaissance. England was a laggard in adopting measures developed on the continent.
In the seventeenth century there were four plague epidemics in Britain. In London these are estimated to have killed 23, 20, 8 and 18% of the population, rebounding each time thanks to migration from the countryside. But the epidemic of 1665–6 was the last.
From the 1730s plague also ceased to be a significant feature in most of Europe. The disappearance of famine and plague from early modern England did not, however, lead to any long-term decrease in overall mortality or increase in the expectation of life.


London plague victims being buried in 1665, one of nine scenes from John Dunstall's Plague broadsheet (1666). Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0)
London plague victims being buried in 1665, one of nine scenes from John Dunstall's Plague broadsheet (1666). Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0)
Mortality worsens in the early modern period
One reason for this was urbanisation accompanied by increased trade, while European expansion across the Atlantic led to the microbial unification of the world, the consequences of which are still very much with us.
This intensified the circulation of disease vectors and introduced novel pathogens to both the ‘old’ and ‘new’ worlds. As a result of these interconnected processes, national life expectancy flat-lined from 1650 to 1750 at levels lower than had prevailed in the less urbanised late sixteenth and early seventeenth centuries.
Higher populations, urbanisation and increased local and global interconnections through trade led to many pathogens becoming permanently present, or endemic, especially in urban populations, rather than raging through periodically as introduced epidemics.
This process of endemicization had three key effects. First, it tended to increase the general level of mortality. Second, diseases which were immunising, came to be predominantly childhood diseases, increasing the chances of dying in childhood, but decreasing the chances of dying at later ages, for those who survived childhood. Third, it made annual patterns of mortality more stable (see figure 4).

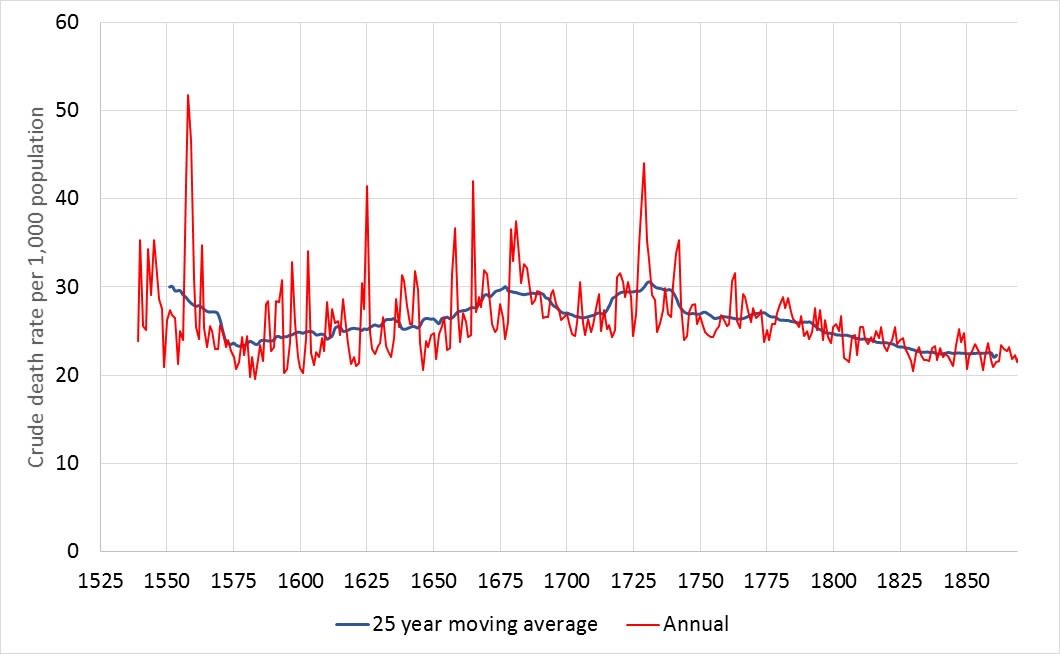
Figure 4: Crude death rate (deaths per thousand population) 1543–1869: Demonstrates the progress of endemicization. Data from Wrigley and Schofield, Population history.
Figure 4: Crude death rate (deaths per thousand population) 1543–1869: Demonstrates the progress of endemicization. Data from Wrigley and Schofield, Population history.
In the epidemic year 1558, deaths were over 80% above normal, and in the plague year 1625, mortality was 65% above the 25 year average. In the sixteenth, seventeenth and early eighteenth centuries, epidemics were frequent – in the 200 years between 1551 and 1749, mortality exceeded the average by 10% or more in 37 years, or one year in five.
For COVID-19 to be this severe in Britain today, deaths from the disease would probably have to go far above 100,000 in a single year.
By contrast, by the early nineteenth century annual fluctuations were generally very modest. Between 1800 and 1869 only in one year, 1847, was mortality 10% or more above trend. This is unmistakable evidence of endemicization.
Death had become more predictable and was increasingly concentrated in childhood years.


Life and death. Oil painting, 18th century. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0)
Life and death. Oil painting, 18th century. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0)
The improvement in life expectancy
Despite ongoing urbanisation overall life expectancies began to rise from the middle of the eighteenth century. One major factor was increasing control over smallpox, which was probably the leading cause of death in mid-eighteenth century England, but only a minor cause of death by the mid nineteenth century. This did not begin with Jenner’s famous discovery of the world’s first vaccine in 1796, important as this was.
In 1718, a different technique had been introduced into England from the Ottoman Empire, by Lady Mary Wortley Montagu. The procedure, termed inoculation, involved administering a small dose of smallpox to the patient via an incision in the skin. In most cases this would lead to a very mild infection and confer immunity – in a small minority it proved fatal.
After 1760, inoculation and the use of quarantine became widespread in southern England. Autonomous mutation of the virus that led to greater infectiousness in the late eighteenth century, together with poor law practices in the rural south – from where most London migrants originated – were probably conjointly responsible for the major reduction in smallpox mortality in the capital amongst adult migrants.
This contributed to the spectacular decline in the excess of deaths over births that occurred over the last three decades of the century.


Rash of pustules on the hand of a patient, probably suffering from smallpox. Watercolour by R. Carswell, 1831. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0)
Rash of pustules on the hand of a patient, probably suffering from smallpox. Watercolour by R. Carswell, 1831. Credit: Wellcome Collection. Attribution 4.0 International (CC BY 4.0)
Vaccination played a major role after 1798. The trend towards an excess of deaths over births appears to have been a general feature of urban centres in England and at least some cities elsewhere in the late eighteenth and early nineteenth centuries.
The most virulent diseases were those which were most easily dealt with. Alongside smallpox, the big killers that declined rapidly across the eighteenth and early nineteenth centuries were malaria and typhus. It was the decline of these diseases, combined with the earlier disappearance of famine and plague, which drew the era of major epidemics to a close.
Malaria is not associated with England today, but areas of extensive marshy wetland, such as the fens, suffered from endemic malaria. Drainage aimed at agricultural improvement were probably largely responsible for the decline in malarial mortality in England.
The second half of the nineteenth century saw major reductions in waterborne diseases as a consequence of widespread improvements in water supply and sewerage.
Most of the long-run improvements to life expectancy in Britain have occurred since 1900, with the largest improvements occurring in the first half of the twentieth century.
Rising living standards and public health interventions played a major part in this. Mortality from tuberculosis and measles, for example, declined enormously, and this probably reflected improving nutritional status and reduced residential crowding.


An x-ray is taken of a young man's chest to look for signs of tuberculosis at Harefield Hospital, Hertfordshire, England, 1943. Credit: Imperial War Museums.
An x-ray is taken of a young man's chest to look for signs of tuberculosis at Harefield Hospital, Hertfordshire, England, 1943. Credit: Imperial War Museums.
The period after about 1950 is where medicine came to make large contributions. This saw the widespread use of antibiotics and mass vaccination campaigns against a whole series of infections.
Smallpox became the first, and to date only, disease to be eradicated from the human population on a global basis. This was achieved as a result of a sustained and coordinated global eradication programme initiated by the World Health Organisation (WHO) in 1959. The last non-laboratory case of smallpox was in 1977 with the disease officially considered eradicated in 1980.
High modern rates of death from cancer and other chronic diseases are not simply the negative consequence of smoking and air pollution. The primary cause is the declining incidence of death from infectious diseases, allowing more and more people to live long enough to succumb to cancer, heart disease, or dementia. Death remains inevitable. Reducing one cause of death inevitably leads to an increase in other causes, typically at later ages.
The dominance of non-communicable disease as a cause of death today is a measure of our success in extending human life by reducing deaths from infectious disease.
In more recent decades, deaths from cancer and heart-disease have also begun to fall.
Globally, improvement to human life expectancy has been remarkably steady over the last 180 years – since 1840 the highest national life expectancy globally has increased by three years in every decade.
Can we learn anything from history?


Perhaps. Predictions about the future are notoriously unreliable but I would venture to make a few observations:
- Like the 1918 flu pandemic, COVID-19 is likely go down in history as a short-term interruption to long improvements in life expectancy, and it is most unlikely that the improving trend in global life expectancy will not resume within a few years.
- There is no road back to some older safer world before the current era of globalisation. That older world was far more deadly than ours in every country in every month of every single year. Nor can we turn back the clock on global inter-connectedness. At least as far back as the Plague of Justinian in the sixth century, epidemics have crossed the Eurasian landmass. From the late sixteenth century, European expansion led to the microbial unification of the world, laying the foundations for truly global pandemics. This cannot be reversed, nor would it be desirable to do so.
- Whilst COVID-19 is highly infectious, when seen in historical context, it has a low case-fatality rate. The best estimates are currently somewhere in the range 0.5 to 1%, and perhaps two-thirds of deaths to COVID-19 are of people who would have died very soon anyway. The case-fatality rate may be a significant overestimate, but it is considerably lower than the 1918 flu pandemic which killed around 50 million people with an average case-fatality rate of around 2.5%.
The case-fatality rate of COVID-19 does not begin to compare with vanquished diseases like plague, smallpox or cholera. The Black Death may have had a case-fatality rate of 60–90% and struck down people of all ages both healthy and not. By the late eighteenth century, smallpox had a case-fatality rate of perhaps 20–30%, but did at least confer life long-immunity. In the nineteenth century, cholera probably had a case fatality rate of 25–50%, killing many of its victims within 24 hours.
When the HIV pandemic struck in the 1980s, before the development of retroviral drugs, the case fatality rate was over 80%. But HIV spread relatively slowly and it rapidly became clear how to minimise the risks. As a result, outside sub-Saharan Africa, and high risk groups elsewhere, the mortality impact of HIV was limited despite the case fatality rate. In 2020, we could easily have been confronted with something as infectious as COVID-19 but far more virulent, though there is an evolutionary trade-off for many pathogens between infectiousness and virulence.
- Sooner or later, another pandemic will occur, and if we are unlucky, it may be far more virulent than COVID-19 but just as infectious. Experts have always known that the world remained vulnerable to novel pathogens or new more lethal strains of old pathogens, but most governments were both woefully underprepared and either unable or unwilling to start making adequate preparations in the first three months of 2020.
COVID-19 may provide a wake-up call to be better prepared in the future, and to fund international agencies, not least the chronically underfunded WHO, at much higher levels, but this is by no means guaranteed. It might even make the world more realistic about the risk of business as usual and failing to take decisive and timely action against the looming existential threat of climate change.
Leigh Shaw-Taylor is Senior Lecturer in History and Co-director of the Cambridge Group for the History of Population and Social Structure.


