Cancer cells can now be viewed as never before, thanks to cutting-edge imaging tools being developed in Cambridge.
Cancer cells can now be viewed as never before, thanks to cutting-edge imaging tools being developed in Cambridge.
Increasing the speed and sensitivity of detecting how tumour cells are responding to treatment is something of a Holy Grail in the field of oncology. Treatment response is still largely assessed by looking for a reduction in tumour size using magnetic resonance imaging (MRI) or X-ray computed tomography. But many tumours may take weeks or even months to show evidence of regression and, in some cases, may not regress at all despite a positive response to treatment. How can an earlier indication of response be achieved so that clinicians can select the best treatment for an individual patient?
New techniques are being pioneered in Cambridge to ‘see’ tumour cells as never before. Research in Professor Kevin Brindle’s laboratory is developing a variety of clinically applicable, non-invasive, imaging techniques that measure tumour cells ‘eating, breathing and dying’.
Spin doctor
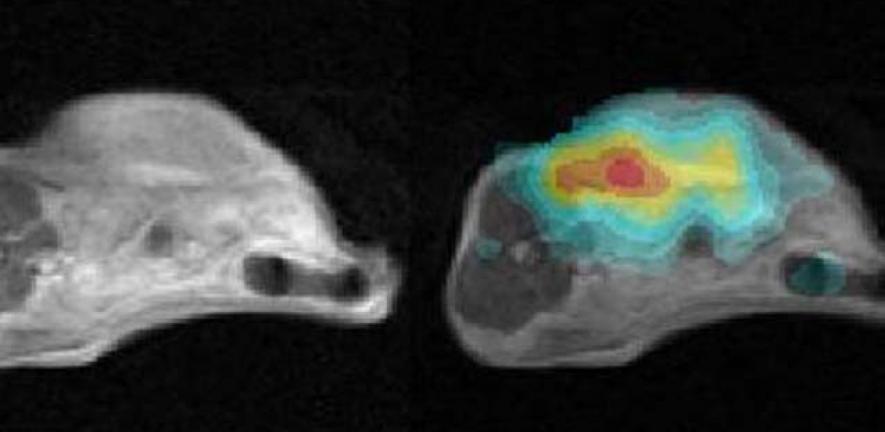
One approach under investigation by the Brindle lab is based on MRI. Although this technique has been around since the 1970s, the new imaging method has a crucial difference – instead of detecting the distribution and properties of water protons in tissue, which conventional MRI does, the new approach detects with much greater sensitivity than ever before the small molecules in tissues that are fundamental to their biochemistry. These are the carbon-based metabolites involved in producing energy and in making the constituents of the cell; a change in how these metabolites are being used can signal that an effective therapy is starting to kill the cells.
The problem with carbon-based molecules is that they are present in tiny amounts compared with the protons in tissue water, making them hard to detect and almost impossible to image at high resolution. To overcome this, the Brindle group has been collaborating with GE Healthcare to develop a technique that increases MRI sensitivity by more than 10,000 times.
To achieve such a dramatic increase in sensitivity, the scientists have turned to nuclear spin hyperpolarisation. Before intravenous injection, a molecule labelled with an MR isotope of carbon is hyperpolarised so that a large proportion of the carbon nuclear spins line up with the magnetic field, as opposed to only a few in a million in a conventional MR experiment. The resulting gain in sensitivity means that the researchers can watch how the hyperpolarised carbon is metabolised by tumours, using this as a read-out for living and dying cells. Data published recently have shown how well this technique works for monitoring treatment response, and the first clinical trials are planned to start in 2010.
Personalising medicine
Different tumours are likely to require different imaging methods. With recent funding from the Leukaemia and Lymphoma Society, a new study has just begun in which several of the imaging methods under development in the Brindle group are being validated in models of lymphoma, so that the best reagents and protocols can be selected for future clinical trials.
Improved imaging methods are not only useful in the clinic, but will also be invaluable for early stage clinical trials of new drugs, where the need to establish whether new treatments are working is particularly acute. Professor Brindle is working with Professor Duncan Jodrell and Dr David Tuveson at the Cancer Research UK Cambridge Research Institute to develop imaging methods that allow treatment responses in individual patients to be measured immediately. Because patients with similar tumour types can show markedly different responses to the same therapy, imaging will be an important component of the armoury of ‘personalised medicine’, enabling the most effective treatment to be tailored to specific patients.
For more information, please contact Professor Kevin Brindle (kmb1001@cam.ac.uk) at the Department of Biochemistry and the Cancer Research UK Cambridge Research Institute/Li Ka Shing Centre. This research was published in Proceedings of the National Academy of Sciences (2009) 106, 19801–19806 and was funded principally by Cancer Research UK, with material support from GE Healthcare.

This work is licensed under a Creative Commons Licence. If you use this content on your site please link back to this page.



